The 21st of November is Stop Pressure Injury Day. Throughout this time we will be raising awareness of pressure injuries by highlighting the global impact they can have on patients and care environments, how they are caused and the best ways to prevent them with a series of informative articles.

Pressure injuries are today included among the daily challenges faced by clinicians around the world and their prevalence and incidence remain high in many care settings.1

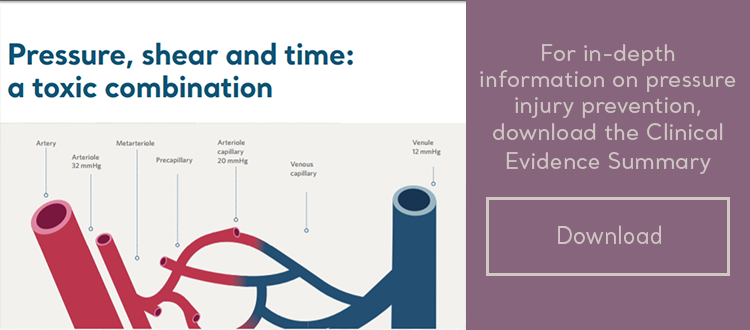
Pressure injuries consist of wounds characterised by localised injury to the skin or underlying tissue, usually over a bony prominence as a result of pressure, or pressure in combination with shear.2 They have a significant humanitarian and economic impact 3,4 with yearly associated costs in the U.S. alone at $11 billion.5
So, what are the top surface technologies than can help you prevent these injuries in care environments?
1. Alternating Pressure Redistribution

Any surface that periodically redistributes pressure, irrespective of patient movement, is deemed to be active1 also called alternating pressure redistribution surface. The argument for high-amplitude pressure redistribution in many cases is compelling. High-amplitude pressure redistribution closely mimics the action of natural spontaneous movement by off-loading several times each hour. This feature, as found in the Auto Logic® mattress replacement system, is particularly important for patients who cannot be repositioned frequently,1 including those treated for intensive care, traction, respiratory, pain, end of life care, and others. Active mattresses are also beneficial from a financial viewpoint as economic studies suggest that active mattresses are both cost-effective6,7 and associated with the greatest risk reduction.8
2. Reactive Pressure Redistribution

Reactive surfaces1 provide an alternative method of pressure redistribution. As opposed to periodic inflation and deflation of air cells in active pressure redistribution, the entire surface of a reactive mattress or cushion yields to the patient’s weight. This allows the body to immerse into, and be enveloped by, the supporting medium: air powered or non-powered, gel or foam. Many reactive surfaces contain a single supporting medium such as foam. Others, such as the AtmosAir® 9000, have a combination of air and foam regulated by Self Adjusting Technology (SAT™) to optimise pressure redistribution, comfort and support without the need of a pump unit. Reactive surfaces, such as the AtmosAir range, have also delivered proven efficacy in a number of field evaluations and trials.9,10,11,12 This has enabled facilities to both reduce the incidence of facility-acquired pressure injuries and reduce the cost of dynamic overlay rental.13
3. Microclimate Management

There are many ways to normalise the local skin microclimate, the easiest being to reposition the patient. This is not always possible, however, and many patients require additional intervention. A powered coverlet designed to fit over an existing active or reactive mattress, like Skin IQ MCM, offers a solution as it applies negative airflow to draw temperature and moisture through a spacer fabric and away from the skin. By having the ability to proactively regulate tissue microclimate, Skin IQ MCM has proven beneficial in normalising microclimate, reducing odour and promoting an environment conducive to healing.14,15,16,17
By better controlling excess moisture and temperature at the patient skin and surface interface, Skin IQ can optimize pressure injury management.
4. Heel Flotation and Wound Off-loading

The heel is particularly susceptible to pressure injury and often in need of specialised protection, and it may be recommended to offer complete and permanent off-loading.1 This can be made possible through Wound Valve™ Technology found in Arjo’s Nimbus range that isolates and permanently deflates air cells in the foot section of the mattress.
5. Posture and Repositioning

Posture and repositioning are key to pressure injury prevention. A 30° maximum backrest elevation is recommended if not medically contraindicated.1
“Avoid head-of-bed elevation or a slouched position that places pressure and shear on the coccyx."1 |
Regular repositioning, the cornerstone of prevention, is most likely to occur when clinicians have immediate access to lifting equipment.18 Besides supplementary repositioning aids, beds such as the Citadel C200 have integrated ‘patient turn’ features to complement the manual repositioning of patients for periodic care procedures, while reducing the physical burden for the caregiver. The Citadel Patient care system also provides a continuous patient turn function which can complement or supplement routine repositioning while allowing the patient to rest.
Effective methodologies to help prevent pressure injuries
Active and Reactive Pressure Redistribution, Microclimate Management, Heel Flotation, together with Posture and Repositioning, are all effective methodologies to help prevent pressure injuries. It is important, however, to match product functionality with individual therapy goals, as well as the care environment, to ensure the right surface for the right patient at the right time.
To learn more about Arjo’s range of pressure injury products, please download the document below.
Choosing the most effective pressure redistribution and Microclimate management solution should be based on a holistic assessment of your patient or resident. Please contact your local Arjo representative to find out which solution can be best tailored to your needs.
References
[1] Arjo Clinical Evidence Summary – Pressure Injury Prevention Solutions.
[2] National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory panel and Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline. Emily Haesler (Ed.). Cambridge Media: Osborne Park, Western Australia; 2014.
[3]Dealey C, Posnett J, Walker A (2012). The cost of pressure ulcers in the United Kingdom. Journal of Wound Care; 21(6):261-266.
[4] Brem H, Maggi J, Nierman D et al. High cost of stage IV pressure ulcers. Am. J. surg. 2010; 200:473-477.
[5] Reddy M et al. JAMA. 2006;296(8):974-984
[6] Iglesias C, Nixon J, Cranny G et al. (2006) Pressure relieving support surfaces (PRESSURE) trial: cost effectiveness analysis. BMJ 2006;332(7555):1413-1415.
[7] Clark M. (2000). Models of pressure ulcer care: costs and outcomes. British Journal of Healthcare Management. 2000; 7(10):412-416.
[8] Trueman P, Whitehead SJ (2010). The economics of pressure relieving surfaces: an illustrative case study of the impact of high specification surfaces on hospital finances. International Wound Journal. 2010;7:4-54.
[9] Newton H (2014). Evaluating a pressure redistribution mattress replacement system. British Journal of Nursing, Suppl 20:s30-35.
[10] Newton H (2015). A 6-month evaluation of a non-powered hybrid mattress replacement system. Br.J Nursing, 11:24(suppl):S32-36.
[11] Bedo J (2013). Reducing hospital acquired pressure damage: An NHS acute trust initiative. British Journal of Nursing, 22(20):S24-S28.
[12] Bed TiME: Non powered hybrid therapy (AtmosAir 4000™) and the impact on patient care, staff, and powered dynamic mattress usage. Poster Presentation: 19th EPUAP Annual Conference, Belfast, Sept 2017.
[13] Beth Israel Medical Centre, NY. Use of self-adjusting technology (SAT) mattress to help reduce a facility’s use of therapeutic overlays. ArjoHuntleigh Case Study on file.
[14] Reger S, ranganathan V, McNulty A (2014). Use of a powered coverlet for moisture removal, skin temperature reduction, odour and bacteria control. J Wound Ostomy Continence Nursing, 41(1)35-39.
[15] Clark M, Lahmann N (2017). Clinical evaluation of the Skin IQ Microclimate Manager and case reports. Wounds International. 2011 (suppl.):1-4. At: http://www.woundsinternational.com/media/issues/533/files/content 10235.pdf accessed August 2017.
[16] Kohr R (2011). Simple solutions for low air loss needs: evaluating a new surface. Poster presentation, 30th CAET National Conference, Montreal, Quebec, May 26th-29th.
[17] Collier M, Potts C, Shaw E (2014). Use of a coverlet system for the management of skin microclimate. British Journal of Nursing (Tissue Viability Supplement 23(15):S28-35.
[18] Phillips L. Pressure ulcer prevention: keep it safe, keep it simple. In: Duffy V, Lightner N (eds). Advances in Human Aspects of Healthcare. Proceedings Applied Human Factors and Ergonomics: USA. 2014; 3: 19-24.
