As patient age and acuity levels continue to rise, increasing frailty, complex underlying chronic diseases and rising obesity add to the daily challenges faced by clinicians. These challenges include pressure injuries; wounds characterised by localised injury to the skin and/or underlying tissue, usually over a bony prominence as a result of pressure or pressure in combination with shear.1

Despite advances in surface technologies, education, guidelines and facility-based continuous improvement programmes, pressure injury prevalence and incidence remains high in many care settings. These injuries have a significant humanitarian and economic impact2,3 but are generally considered avoidable4 if pressure, shear, time and microclimate are effectively managed.
1. The pyramid of care
The pyramid of care focuses on key factors that can lead to pressure injury if they are not managed appropriately.

Within the pyramid, interventions should be prioritised towards the factors that can be easily modified but are likely to have the biggest impact on the prevention of pressure injury.
Once interventions focused on the more basic risk factors have been prioritised, such as pressure and moisture, the more complex risk factors can be addressed.
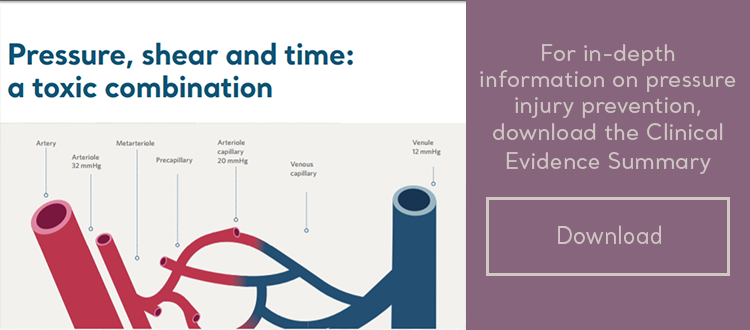
2. Pressure and shear

While pressure may be applied directly to the skin, the effects of pressure are frequently exacerbated by lateral shear forces. This is primarily due to the impact of posture and soft tissue deformation, which result in the compression, distortion and occlusion of small blood and lymph vessels. The interrupted supply of oxygen and micronutrients, combined with the failure to remove toxic metabolites, can potentially lead to tissue ischaemia and irreversible necrotic injury.1
3. How much pressure is safe?
Studies have shown that pressure as low as 6mmHg is sufficient to occlude the microcirculation.5,6 However, there is also an inverse relationship between pressure and time.7
While there is no ‘safe’ pressure for every individual, it is evident that tissue can withstand higher pressure for short periods or lower pressure for longer periods, with muscle being most susceptible to damage.
4. Tissue tolerance
The evolution of a pressure injury also depends upon individual tissue tolerance; this is affected by many physical and environmental risk factors. While the exact importance of most risk factors is yet to be elucidated1 and not all can be modified (such as age and underlying disease), the importance of other factors, such as excess heat and moisture on the skin, has been clearly defined through contemporary research.
5. Tissue environment
If the temperature at the skin rises by just 1°C, the resultant hyperaemic response increases metabolic demand. This increase can occur at a time when the blood supply may be limited by vessel occlusion through pressure and shear. This can be particularly problematic when higher pressure are experienced8, and pressure alone can trigger a temperature rise.9
At the same time, increased heat may trigger a natural sweat response and create a continually moist environment. Moisture reduces the tensile strength of the skin, leading to maceration1 and an increased risk of friction damage.
“Increased heat may trigger a natural sweat response and create a continually moist environment. |
Effective methodologies to help prevent pressure injuries
Prevention begins with the identification of individuals at risk as early as possible in the care pathway, and then taking prompt action to provide the correct intervention1,10 which may include early mobilisation.1
Unfortunately, it will never be possible to address all risk factors. It is, therefore, important to prioritise the interventions most likely to have the greatest impact on clinical outcomes, primarily: pressure, shear and microclimate.11
As a priority, vulnerable patients are typically allocated a therapeutic support surface for their bed and chair. As not all surfaces perform in the same way, and patient tissue tolerance varies, it is important to match the right surface to the right patient at the right time, according to clinical need.1
Whilst the collective features and corresponding performance of a specialised surface vary considerably, all redistribute pressure either by generating a constant low-pressure environment (reactive surface) or by periodically lowering pressure through the deflation of alternating air cells (active surface). In addition, many surfaces also feature in-built microclimate management (low air loss) systems, or can be fitted with a microclimate management coverlet, such as Skin IQ® MCM.
Selecting a support surface
Therapy support surface technologies represent one element of a pressure injury prevention programme. While a pressure redistribution mattress may enable the repositioning regimen to be individualised, regular postural change is still important but not without risk to the patient or the caregiver.
The provision of effective pressure redistribution and microclimate management solutions should be based on a holistic assessment of your patient or resident.
It is important to match product functionality with individual therapy goals, as well as the care environment, to ensure the right surface for the right patient at the right time.
This approach may help to prioritise scare resources and interventions to those who are likely to benefit the most.
Choosing the most effective pressure redistribution and Microclimate management solution should be based on a holistic assessment of your patient or resident.
Please contact your local Arjo representative to find out which solution can be best tailored to your needs.
References
- National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance. (2014). Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline. Emily Haesler (Ed.). Cambridge Media: Osbourne Park, Western Australia.
- Dealey C, Posnett J, Walker A. (2012). The Cost of Pressure Ulcers in the United Kingdom. Journal of Wound Care. 21(6):261-266.
- Brem H, Maggi J, Nierman D et al. (2010). High Cost of Stage IV Pressure Ulcers. Am J Surg. 200:473-477.
- AHRQ. (2017). Never Events. Available at: https://psnet.arhq.gov/primers/primer/3/never-events Accessed August 2017
- Williams SA, Wasserman S, Rawlinson DW. (1998). Dynamic Measurement of Human Capillary Blood Pressure. Clinical Science. 74:507-512.
- Landis EM. (1930). Micro-Injection Studies of Capillary Blood Pressure in Human Skin. Heart. 15:209-228.
- Gefen A, Van Nierop B DL et al. (2008). Strain-Time Cell Death Threshold for Skeletal Muscle in Tissue-Engineered Model System for Deep Tissue Injury. Journal Biomechanics. 41(9):2003-2012.
- Lachenbruch C, Tzen YT, Brienza DM et al. (2013). The Relative Contributions of Interface Pressure, Shear Stress and Temperature on Tissue Ischaemia: A Cross Sectional Pilot Study. Ostomy Wound Manage. 59(3):25-34.
- Angelidis L, Lidman D, Sjaberg F. (2009). Decubitus Ulcer Development: Pressure Alone Increases Tissue Temperature. Europ Journ Plast Surg. 32(5):241-242.
- Pressure Ulcer Point Prevalence Survey: Statewide Report. (2006). Victorian Public Health Service, Victoria, Australia. Available at: https://www.2.health.vic.gov.au/about/publications/researchandreports/pressure-ulcer-prevalence-survey accessed August 2017.
- Phillips L. (2014). Support Surfaces: Taking the Pressure out of Pressure Ulcers. British Journal of Nursing. Ed Cowan T. MA Healthcare Ltd.
